INTRODUCTION
Pain, which is often inadequately treated, accompanies most of the surgical procedures performed and persists long after tissue heals. It is estimated that pain is insufficiently treated in approximately 50% of all surgical procedures.1 Management of early postoperative pain is the most common concern after the elective laparoscopic cholecystectomy.2
Pregabalin is a structural analogue of gamma-aminobutyric acid that acts as a potent ligand for alpha 2-delta subunits of the voltage-gated calcium channels in the nervous system. Such action results in a reduction in the depolarisation-induced influx of calcium, hence a reduction in the release of excitatory neurotransmitters, including glutamate, noradrenaline, dopamine, and serotonin. Pregabalin and more potent than gabapentin and has fewer adverse effects than gabapentin and has a linear pharmacokinetic profile.3 All these characteristics make pregabalin a suitable adjuvant for preoperative analgesia and can be taken empty stomach, does not lead to gastrointestinal bleeding and is generally well-tolerated.4
A multimodal analgesic technique is now often used in acute postoperative pain management to improve the analgesic efficacy and reduce the total requirement of opioids, which have undesirable adverse effects. Pregabalin is used not only for managing neuropathic pain but also in multimodal strategies for controlling post-operative pain.5
Several studies have demonstrated the efficacy of pregabalin in managing acute post-operative pain. A meta-analysis suggested that pregabalin, at all doses, has an opioid-sparing effect and reduces pain scores in the postoperative setting,6 but it is associated with increased sedation and visual disturbances; however, the efficacy of pregabalin in providing such benefits during laparoscopic cholecystectomy remains uncertain. Clinical studies report that a single pre-emptive dose of 150 mg of pregabalin before LC reduces early postoperative pain scores, decreases opioid consumption by 30-40%, and improves sedation quality without significant adverse effects. For instance, a randomised controlled trial (RCT) by Jokela et al. (2008) demonstrated that 150 mg pregabalin preoperatively lowered 24-hour morphine use by 38% and reduced dynamic pain scores. However, conflicting evidence exists for low doses. Studies like Peng et al. conducted a randomised controlled trial using low-dose pregabalin (50 mg and 75 mg),7 which found only modest early pain relief, with no significant reduction in overall analgesic use, reflecting the limited value of low-dose pregabalin as a stand-alone pre-emptive analgesic.2,8,9,10 None of these studies have demonstrated the efficacy of preemptive single-dose administration of pregabalin in managing postoperative pain in laparoscopic cholecystectomy.7,8 This study aimed to assess the effectiveness of a preemptive single dose of pregabalin in reducing post-operative pain. Pain levels were measured using the Visual Analogue Scale (VAS) at various time intervals: 2, 4, 6, 8, 12, and 24 hours. Total diclofenac consumption was evaluated over 24 hours. While preemptive analgesia is effective in managing pain following various types of surgery, there is limited evidence regarding the preemptive administration of pregabalin before laparoscopic cholecystectomy.
Thus, the purpose of this study is to evaluate the efficacy and safety of a single dose preemptive administration of pregabalin (150 mg) in reducing postoperative pain and nonsteroidal anti-inflammatory (NSAID) drugs in patients undergoing laparoscopic cholecystectomy.
METHODS
Study design
This was a prospective, comparative study designed to assess the efficacy of preemptive pregabalin for reducing postoperative pain and NSAID in patients undergoing laparoscopic cholecystectomy under general anaesthesia.
Participants
A total of 70 adult patients (18-60 years) of either sex, with ASA physical status I or II, undergoing elective laparoscopic cholecystectomy, were analysed in the study. The study was conducted between December 2024 to May 2025 at a tertiary care hospital. Informed consent was obtained from all patients, and the study protocol was approved by the Institutional Ethics Committee (IEC) (IEC/AIMS & RC/2025/343).
Inclusion criteria
- – Adults aged 18-60 years.
- – ASA physical status I or II.
- – Scheduled for elective laparoscopic cholecystectomy under general anaesthesia.
- – Written informed consent obtained.
Exclusion criteria
- – Compromised kidney or liver function (e.g., creatinine > 1.5 mg/dL, ALT/AST > 3x normal).
- – History of drug, alcohol, or opioid abuse.
- – Uncontrolled medical diseases (e.g., diabetes mellitus, hypertension).
- – Pregnant or lactating women.
- – History of NSAID intake within 24 hours before surgery.
- – Neurological disorders or hypersensitivity to pregabalin.
Patients were randomly assigned to one of two groups: pregabalin 150 mg or placebo (blank pregabalin capsules) in a 1:1 ratio using a computer-generated random number table. A staff nurse, not involved in the study, administered the medications 2 hours before the surgery with 1 to 2 sips of water. The study was double-blind, meaning both the patients and the researchers (including those performing pain assessments) were blinded to group allocation.
- – Pregabalin group: received 150 mg of pregabalin orally, 2 hours before the induction of surgery.
- – Placebo group: received an identical blank pregabalin capsule placebo orally, 2 hours before surgery.
Anaesthesia protocol
The anaesthesia protocol was standardised across all groups:
- – Induction: fentanyl (3 μg/kg) and propofol (2 mg/kg).
- – Intubation: facilitated vecuronium (0.08 mg/kg).
- – Maintenance: propofol (100-200 μg/kg/min) and 66% nitrous oxide in oxygen.
- – Reversal: neostigmine (0.05 mg/kg) and glycopyrrolate (0.01 mg/kg) were administered to reverse neuromuscular blockade.
Upon recovery, extubation was performed, and patients were transferred to the Post-Anaesthesia Care Unit (PACU).
Postoperative analgesia
In the PACU, patient-controlled analgesia (PCA) was used with intravenous fentanyl delivered at 20 μg per activation, with a 5-minute lockout period and a ceiling dose of 2 μg/kg/h.
Outcome measures
- – Primary outcome: postoperative pain severity, assessed at multiple intervals (2, 4, 6, 8, 12, and 24 hours) using the Visual Analogue Scale (VAS), where 0 represents no pain and 10 represents the worst imaginable pain.
- – Secondary outcomes:
- Postoperative nausea and vomiting (PONV) incidence.
- Sedation level assessed using the Modified Ramsay Sedation Scale.
- Total diclofenac consumption over 24 hours.
- Rescue analgesic use (in the form of diclofenac or other rescue medications).
Pain assessment was done by an independent volunteer from the anaesthesia department, blinded to the group allocation.
Sample size calculation
To determine the required sample size for our study, we used the standard formula for comparing two groups with continuous outcomes. The calculation included a significance level of 0.1, giving us a Z value of 1.645, and a power of 85%, corresponding to a Z value of 1.036. Based on previous studies, we used a standard deviation of 2.2 and aimed to detect a minimum difference of 1.0 in VAS scores between groups.10
After applying the values, the required sample size came out to be approximately 35 patients in each group, giving us a total of 70 participants.”
Statistical analysis
- – Descriptive statistics: continuous variables were analysed using mean ± standard deviation (SD), and categorical variables were presented as frequencies and percentages.
- – Comparative analysis:
- One-way ANOVA for continuous variables.
- Chi-square test for categorical variables.
- Mann-Whitney U test for VAS scores.
- Student’s t-test for fentanyl consumption.
- Fisher’s exact test for the analysis of side effects.
- – p values less than 0.05 were considered statistically significant. Statistical analyses were conducted using SPSS version 25.0.
RESULTS
A total of 80 patients were assessed for eligibility from December 2024 to June 2025; 100% of patients completed the study. Two groups are randomly assigned to the placebo and pregabalin 150 mg. A total of 70 patients were randomised in the study, with a mean age ± S.D (in years) of 39.97 ± 12.31, of which most of the population were female (n = 44, 62.9%) and the remaining were male (n = 26, 37.1%). The average weight of participants was observed to be 63.92 kg (Table 1).
Table 1. Demographic characteristics of patients (n = 70)
| Demographic variables | Frequency | % | Mean ± S.D. |
|---|---|---|---|
| Age (years) 20-29 30-39 40-49 50-59 Total | 32243270 | 4.331.461.42.9100.0 | 39.97 ± 12.31 |
| Gender Male Female | 4426 | 62.937.1 | |
| Weight (kg) 50-59 60-69 70-79 | 272122 | 38.63031.4 | |
|
Age is reported as both categorical and continuous (mean ± standard deviation). Gender and weight categories are reported in frequency and percentage. The category “50-59” listed under “Gender” in earlier versions appears to be a misplaced value and has been omitted from this corrected table. |
|||
There was no difference among the groups about age, weight, sex, duration of anaesthesia, duration of surgery, and intraoperative fentanyl consumption. Total post-operative pain score is reduced in the pregabalin group, total consumption of diclofenac is significantly reduced in the pregabalin group, whereas the requirement of rescue analgesic is needed in all patients of the pregabalin group. Post-operative nausea and vomiting are also reduced in the pregabalin group compared to the placebo group.
DISCUSSION
In our study, preemptive 150 mg single-dose pregabalin significantly reduced postoperative pain and NSAID consumption, demonstrating its potential as an effective part of multimodal analgesia protocols in laparoscopic cholecystectomy. This result is consistent with previous studies that have shown pregabalin’s effectiveness in reducing postoperative pain and opioid use after surgery.11,12
The pain scores measured by VAS were significantly lower in the pregabalin group at all postoperative time points (2, 4, 6-, 8-, 12-, and 24-hours, Figure 1), which aligns with findings from Patel et al. who observed similar reductions in pain in patients receiving pregabalin for postoperative analgesia12 also the Mann-Whitney U test results show a reduced rank sum in the pregabalin group, indicating reduced postoperative pain compared to the placebo (Table 2). The analgesic effect of pregabalin is likely due to its mechanism of action, where it binds to the α2δ subunit of voltage-gated calcium channels, thereby inhibiting the release of excitatory neurotransmitters like glutamate and substance P.13 This central mechanism of action makes it particularly useful in multimodal pain management strategies, where it complements the effects of NSAID and opioids.14
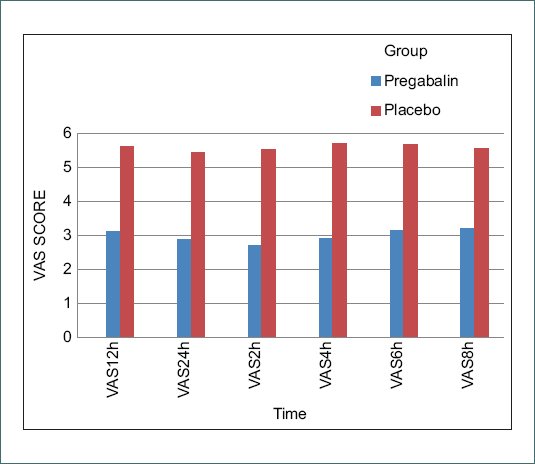
Figura 1. Postoperative pain: pain is expressed as median VAS scores. pregabalin vs placebo by Mann-Whitney U-test. Note. The pregabalin group consistently demonstrated significantly lower VAS scores at all time points compared to the placebo group (P < 0.05). VAS: visual analogue scale.
Table 2. Comparison of VAS score & consumption of diclofenac in pregabalin and placebo group
| Groups | n | Mean rank | Sum of ranks | |
|---|---|---|---|---|
| VAS 2h | Pregabalin | 35 | 18.57 | 650.00 |
| Placebo | 35 | 52.43 | 1835.00 | |
| Total | 70 | |||
| VAS 4h | Pregabalin | 35 | 18.50 | 647.50 |
| Placebo | 35 | 52.50 | 1837.50 | |
| Total | 70 | |||
| VAS 6h | Pregabalin | 35 | 18.86 | 660.00 |
| Placebo | 35 | 52.14 | 1825.00 | |
| Total | 70 | |||
| VAS 8h | Pregabalin | 35 | 19.60 | 686.00 |
| Placebo | 35 | 51.40 | 1799.00 | |
| Total | 70 | |||
| VAS 12h | Pregabalin | 35 | 19.26 | 674.00 |
| Placebo | 35 | 51.74 | 1811.00 | |
| Total | 70 | |||
| VAS 24h | Pregabalin | 35 | 19.03 | 666.00 |
| Placebo | 35 | 51.97 | 1819.00 | |
| Total | 70 | |||
| Total diclofenac consumption (mg) | Pregabalin | 35 | 21.30 | 745.50 |
| Placebo | 35 | 49.70 | 1739.50 | |
|
Data represent mean ranks and sum of ranks derived from the Mann-Whitney U test comparing postoperative pain scores (VAS) and total diclofenac consumption between the pregabalin and placebo groups. In all comparisons, the pregabalin group showed significantly lower VAS scores and diclofenac consumption than the placebo group (p < 0.05). n: number of patients per group. |
||||
Our findings also showed a significant reduction in diclofenac consumption in the pregabalin group (P < 0.001, Table 3), which supports the hypothesis that pregabalin may reduce the need for additional analgesics postoperatively. This result mirrors the meta-analysis by Mishra et al., which found that pregabalin reduced opioid consumption across a variety of surgical procedures.15 The opioid-sparing effect of pregabalin is particularly important given the gastrointestinal, renal, and respiratory side effects associated with opioids.16
Table 3. Results of Mann-Whitney U Test comparing postoperative VAS scores and total diclofenac consumption between pregabalin and control groups
| VAS 2h | VAS 4h | VAS 6h | VAS 8h | VAS 12h | VAS 24h | Total diclofenac consumption (mg) | |
|---|---|---|---|---|---|---|---|
| Mann-Whitney U | 20.00 | 17.5 | 30.0 | 56.0 | 44.0 | 36.0 | 115.50 |
| Wilcoxon W | 650.0 | 647.5 | 660.0 | 686.0 | 674.0 | 666.0 | 745.50 |
| Z | –7.08 | –7.15 | –6.9 | –6.69 | –6.82 | –6.89 | –6.30 |
| Asymp. Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
|
Mann-Whitney U test results comparing Visual Analogue Scale (VAS) scores at various postoperative time points and total diclofenac consumption between the pregabalin and placebo groups. The pregabalin group showed significantly lower pain scores and diclofenac use at all time points (p < 0.001). Wilcoxon W refers to the sum of ranks for the pregabalin group. Z: standard score; Sig.: significance level (2-tailed). |
|||||||
Furthermore, the incidence of postoperative nausea and vomiting (PONV) was significantly lower in the pregabalin group (P = 0.000). This finding is in agreement with Kumar et al., who also found a reduced incidence of PONV (Tables 4 and 5) in patients receiving pregabalin post-surgery.17 While pregabalin is not typically classified as an antiemetic, its ability to reduce opioid consumption may explain the reduction in nausea and vomiting observed in our study.
Table 4. Incidence of nausea in pregabalin and placebo groups
| Nausea | Total | ||
|---|---|---|---|
| No | Yes | ||
| Groups Pregabalin Placebo | 3016 | 519 | 3535 |
| Total | 46 | 24 | 70 |
|
Comparison of the incidence of postoperative nausea between the pregabalin and placebo groups. A significantly lower number of patients in the pregabalin group experienced nausea compared to the placebo group (χ² = 13.62, df = 1, p < 0.001). Percentages not shown for brevity. |
|||
Table 5. Incidence of vomiting in pregabalin and placebo groups
| Vomiting | Total | ||
|---|---|---|---|
| No | Yes | ||
| Groups Pregabalin Placebo | 3327 | 28 | 3535 |
| Total | 60 | 10 | 70 |
|
Comparison of the incidence of postoperative vomiting between the pregabalin and placebo groups. Fewer patients in the pregabalin group experienced vomiting compared to the placebo group (χ² = 4.80, df = 1, p = 0.028). |
|||
Additionally, side effects commonly associated with pregabalin, such as sedation and dizziness, were minimal in our study. This finding aligns with Lee et al., who also observed that a single dose of pregabalin was well tolerated in a variety of surgical populations.18 The absence of significant adverse events suggests that pregabalin could be safely incorporated into preoperative analgesia protocols for patients undergoing laparoscopic surgery.
Limitation
This study suggests that a single preemptive dose of pregabalin can reduce postoperative pain and the need for rescue analgesia, but several limitations must be acknowledged. The follow-up was limited to the first 24 hours of post-surgery, which does not address long-term outcomes like persistent pain or delayed side effects. Only one preoperative dose was assessed, limiting the understanding of pregabalin’s potential with different regimens or in combination with other analgesics, as all patients received the same rescue medication, diclofenac.
The study focused on laparoscopic cholecystectomy, a minimally invasive procedure, so findings may not apply to more painful surgeries. Furthermore, specific patient groups, such as the elderly and those with other health issues, were excluded, affecting the generalizability of the results. Pain was measured using VAS, which is subjective, and common side effects of pregabalin were not formally evaluated. Despite these limitations, the study offers valuable insights into the benefits of preemptive pregabalin for postoperative pain management.
CONCLUSION
In this study, preemptive 150 mg single-dose pregabalin significantly reduced postoperative pain and the incidence of nausea and vomiting in patients undergoing laparoscopic cholecystectomy. These findings suggest that pregabalin may be an effective addition to multimodal analgesia protocols, improving recovery and minimising opioid-related side effects in the West Indian population, particularly in Rajasthan. Future studies should explore its long-term efficacy and generalizability across diverse populations.
DATA AVAILABILITY
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The data will be made available to qualified researchers for non-commercial purposes only, subject to ethical and privacy considerations. Due to privacy restrictions, participant data cannot be publicly shared, but can be accessed by contacting the corresponding author
AUTHOR CONTRIBUTIONS
G. Dewasi, S. Jain and M. Saraf collected the data under the guidance of J. Singh Vaghela, G. Dewasi analysed the data and prepared the final manuscript and submitted it.
FUNDING
None.
CONFLICTS OF INTEREST
None.
ETHICAL CONSIDERATIONS
Protection of humans and animals. The authors declare that the procedures followed complied with the ethical standards of the responsible human experimentation committee and adhered to the World Medical Association and the Declaration of Helsinki. The procedures were approved by the institutional Ethics Committee.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from patients, and received approval from the Ethics Committee. The SAGER guidelines were followed according to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing of this manuscript
